Does the US public support ultraviolet germicidal irradiation technology for reducing risks from pathogens?
Summary
Ultraviolet germicidal irradiation technology (UVGI) or germicidal UV light (GUV) represents a promising technology for reducing catastrophic biorisk and would likely confer near-termist benefits as well
Two subtypes of UVGI, upper-room UVC and far-UVC, seem like particularly promising ways to reduce indoor pathogen transmission.[1]
Understanding the level of support for and awareness of these technologies, what framings of benefits are most compelling, and what concerns exist should be helpful for developing strategies around advocacy and expanding deployment.
We ran four online surveys in November and December 2022 to better understand US public attitudes towards these technologies. As far as we know, these were the first surveys done on US public attitudes towards GUV light as a means of reducing risks from pathogens.
The results of these surveys seem to confirm and disconfirm intuitions in the biosecurity/indoor air quality community around public attitudes towards GUV technology.
Survey results show moderate awareness of GUV light and low awareness of far-UVC light.
Despite low levels of awareness, once respondents were provided with a description of the technology, support for GUV light and its subtypes was broadly positive.
Safety concerns seem to be a meaningful factor in public perception of this technology. Respondents’ most prominent concern was that GUV lights need additional testing to establish more evidence on safety and efficacy.
Contrary to the assumption in the indoor air quality community that since far-UVC involves direct light exposure to humans, people are less likely to support it, we find respondents consistently showed slightly greater support for far-UVC over upper-room UVC.
Also, contrary to the view that terminology for GUV light that includes UV will get less support due to UV’s association with cancer (e.g., far-UVC vs low-wavelength light), our survey shows no statistically significant difference in support when using terms that mention UV vs don’t mention UV.
The attitudes expressed by poll respondents in response to broad questions may not be reliable indicators of actual support for specific policies or messages. It would be better to test people’s responses to more detailed messages and policy proposals
There are further investigations that can be done to tease out different explanations for some of the main findings mentioned in the write-up, to find out whether these results hold across countries, and to gauge public support for indoor air quality more generally.
Methods
We ran four online surveys in November and December 2022. In survey 1, respondents were asked whether they had previously heard of ‘germicidal UV’ (GUV) and ‘far UVC’ as ways to reduce pathogen transmission. They were also asked to provide an open comment on what they currently knew about both technologies.
In survey 2, respondents were presented with a description of germicidal UV light and asked to consider how positively or negatively they felt about the technology for reducing pathogen transmission, the extent to which they would support efforts to deploy germicidal UV in public spaces, and what benefits and concerns they had about this technology.
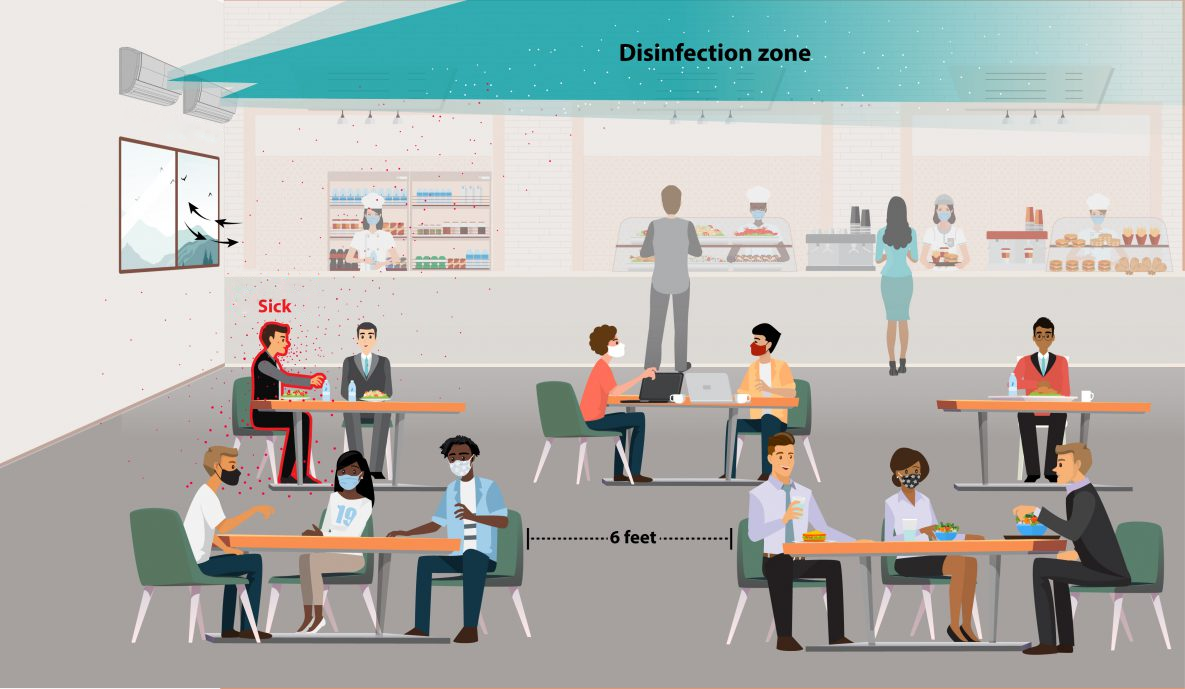
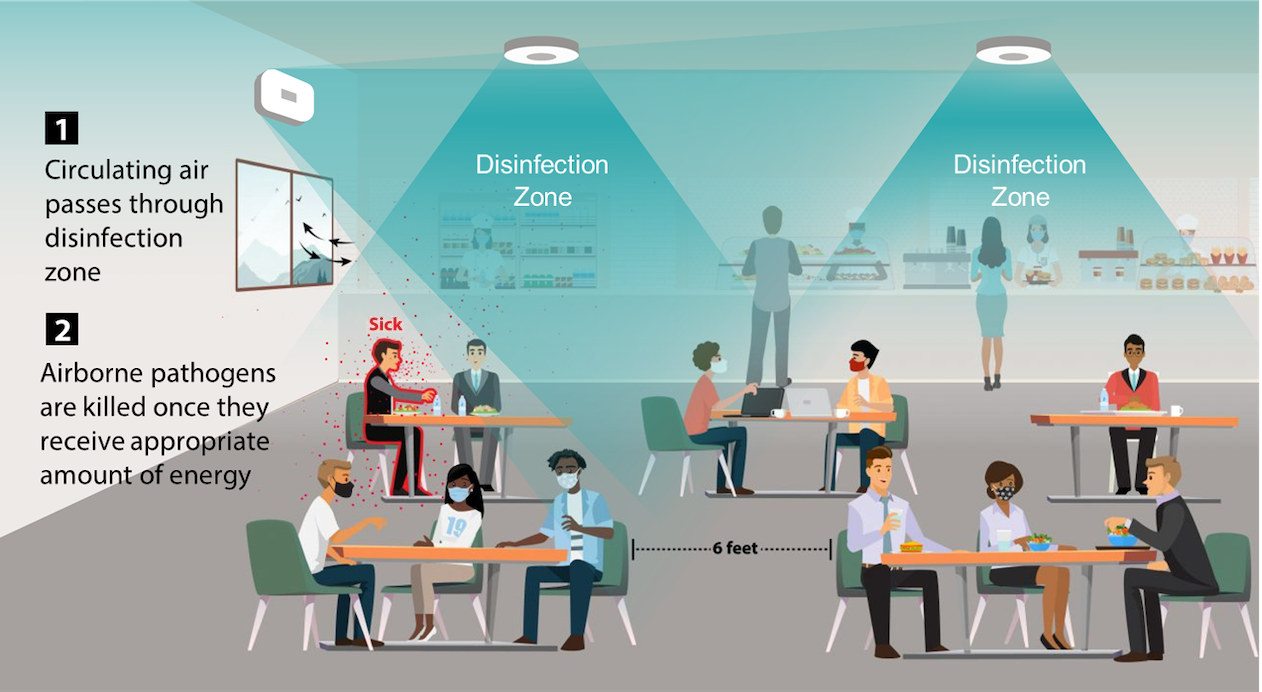
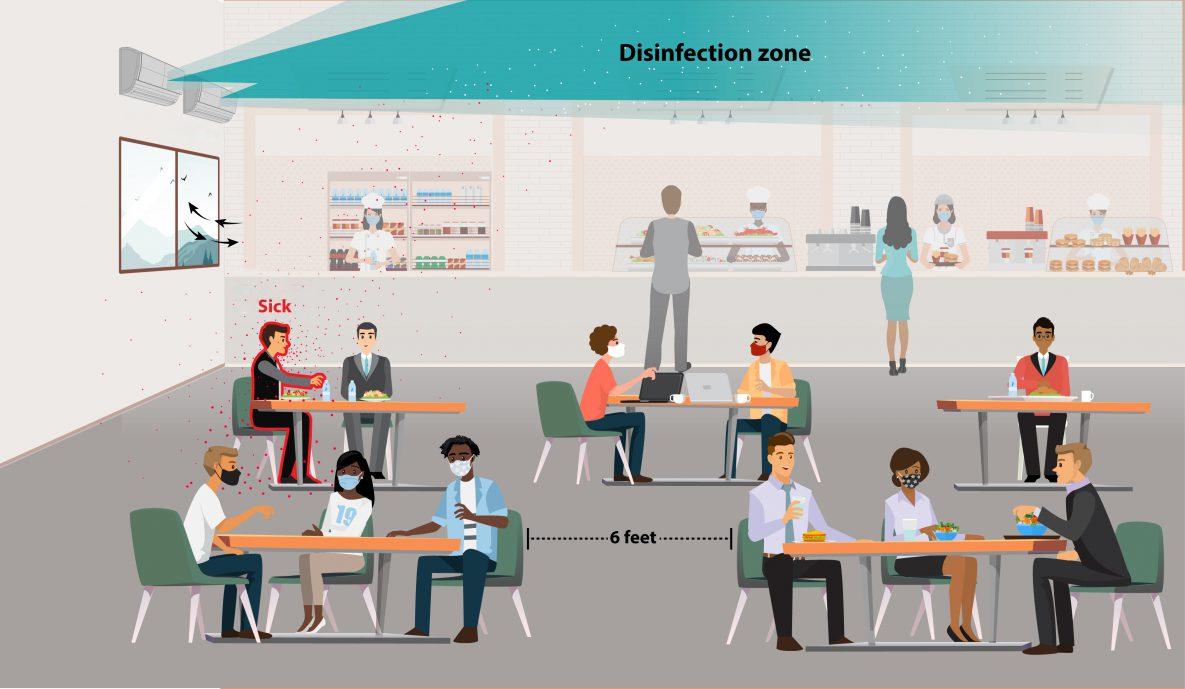
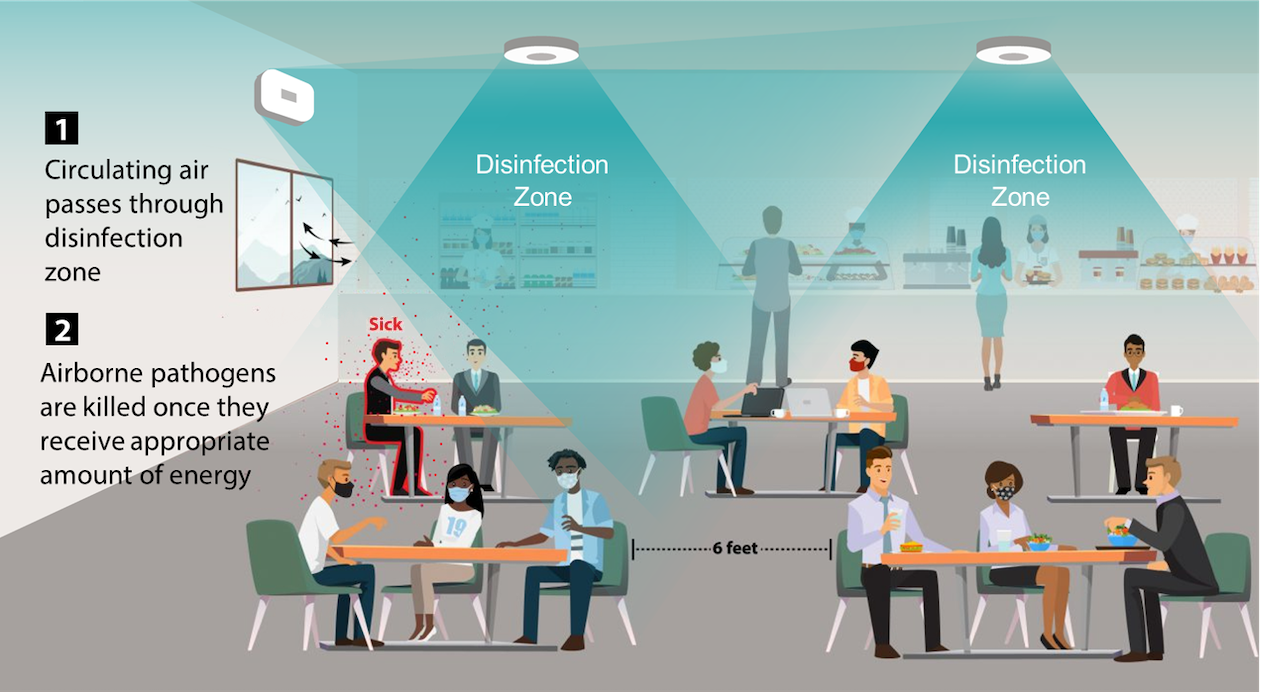
In survey 3, we tested people’s support for three different types of UV light: germicidal UV, far-UVC, and upper-room UVC. We also tested whether including diagrams for far-UVC and upper-room UVC would affect peoples’ support (Figures 1 and 2 below).
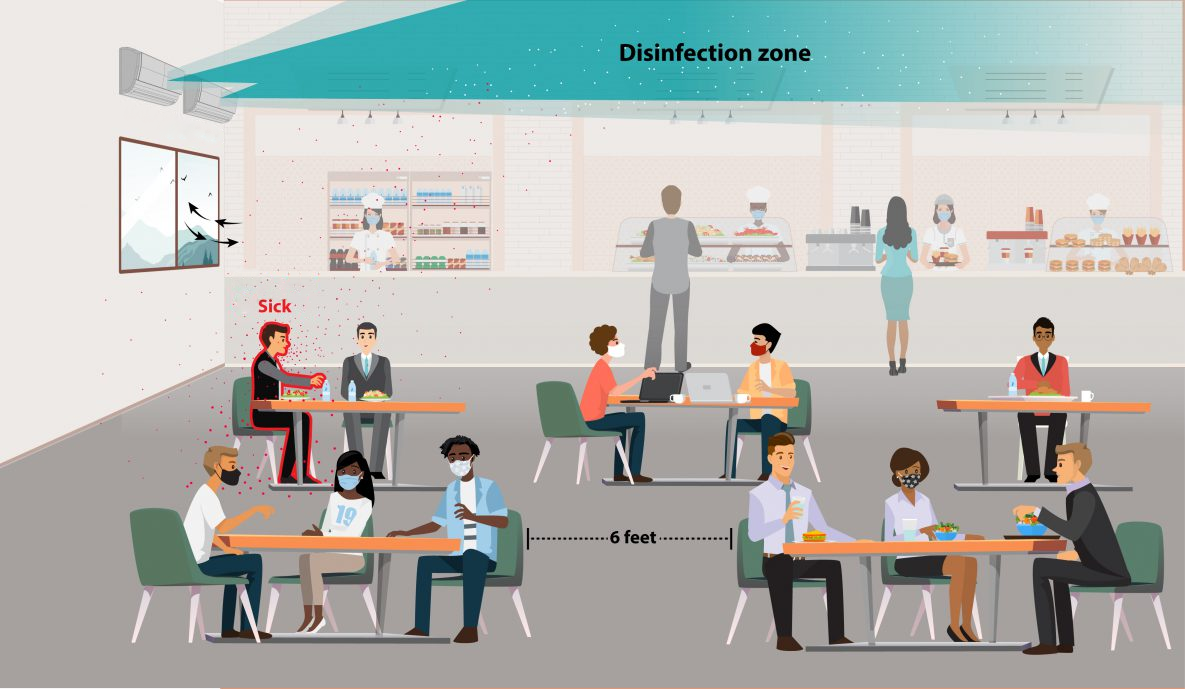
Figure 1: Diagram illustrating use of an upper room UVC system [image provided by Far UV Technologies Inc.]
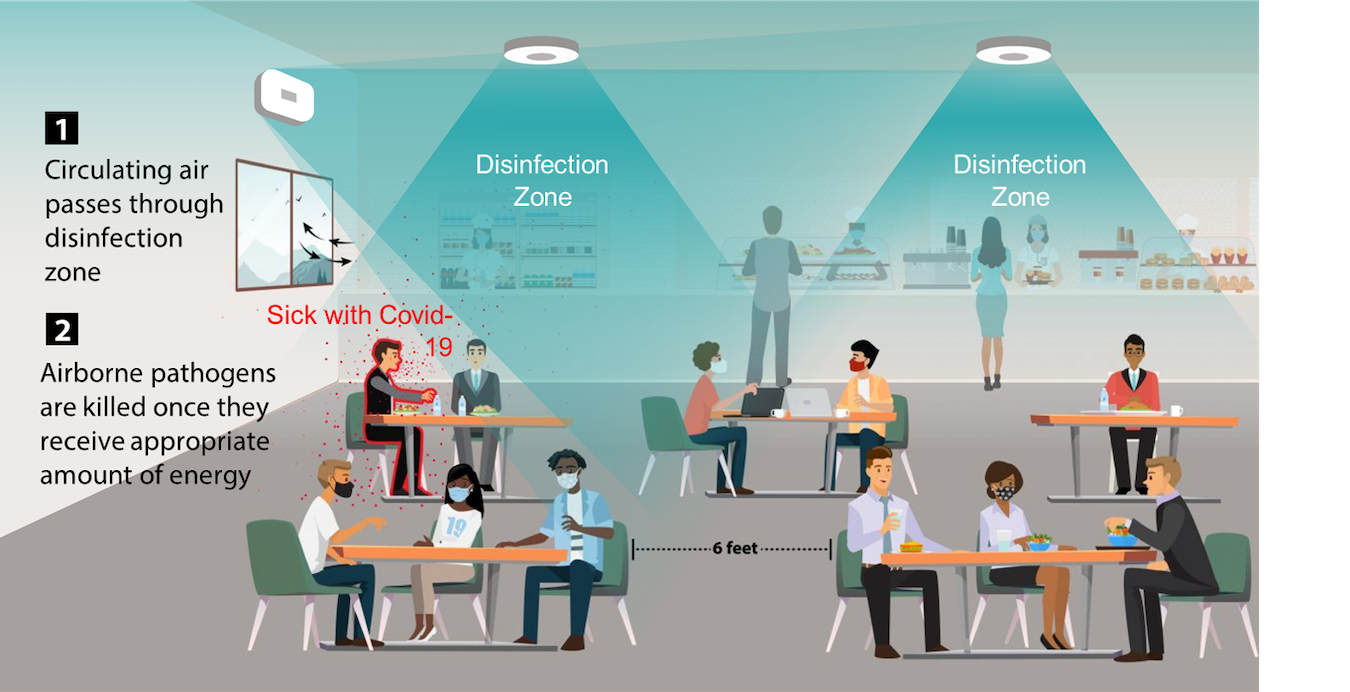
Figure 2: Diagram illustrating use of a far-UVC system [image provided by Far UV Technologies Inc.]
In survey 4, we tested the effect of five different messages on people’s support for three different types of UV light: germicidal UV, far-UVC, and upper-room UVC. We additionally manipulated whether the lights were referred to as germicidal UV, far-UVC, and upper-room UVC lights or germicidal, low wavelength germicidal, and upper room germicidal light.
Respondents were recruited using Prolific and Cint for surveys 1 and 2, and just Prolific for surveys 3 and 4. The survey was administered using Qualtrics. Data were analyzed using R with RStudio.[2] Respondents were from the USA and aged 18 and above. Respondents recruited through Prolific were paid $0.55 USD for completing surveys 1, 3, and 4 and $1.28 USD for completing survey 2. Respondents recruited through Cint were paid as well, but the amount varied depending on what panel they were from, and this was not disclosed to us.
Results: Attitudes towards ultraviolet germicidal irradiation for reducing pathogen transmission
In survey 1, with a sample of 1,289 respondents, weighted to be representative of the US:
We found just under half of the respondents 48.5% (95% CI [42.1%-55.0%]) report they have heard of germicidal UV, while 39.1% (95% CI [33.1%, 45.3%]) say they have not heard of it, with the rest being not sure.
We found 60.9% (95% CI [52.9%, 68.3%]) have not heard of far-UVC, with only 18.7% (95% CI [12.9%, 26.2%]) saying they have, the rest being not sure.
On the whole, we would expect the numbers claiming to have heard of anything to be inflated (because people like to appear knowledgeable and lean towards claiming to have heard of things if they have any doubt), so the true number is probably lower.
In the open comments, people don’t seem to know much about the technology (as we would expect). Many people seem to know about it only in the context of being used to clean gadgets/devices.
Survey 2 had a sample of 1,941 respondents, weighted to be representative of the US:
Overall, support for GUV light as a biodefense measure was very high.
81.1% (95% CI [77.0%, 84.6%]) of the respondents reported positive feelings about using GUV light to reduce pathogen transmission, with only 6.21% (95% CI [4.03%, 9.44%]) reporting negative feelings.
81.2% (95% CI [77.1%, 84.7%]) supported GUV light in buildings they used (e.g., offices, schools, businesses)
A slight majority of respondents (54.87%, 95% CI [49.9%, 59.6%]) answered that they felt the technology was safe or very safe based on what they currently know, with the rest answering that it was slightly safe or not safe.
Respondents were broadly supportive of using GUV light in different public buildings (see Appendix item I).
They were most in favor of using these lights in hospitals (82.49%, 95% CI [77.8%, 86.3%]) and least in favor of using them in schools (75.7%, 95% CI [70.7%, 80.1%]).
We looked at level of agreement for different possible benefits from germicidal UV. Reducing risks for vulnerable people was rated as the most significant benefit (M=7.64, 95% C [7.13, 7.81]), followed by reducing the risk of society-wide pandemics (M=7.51, 95% CI [7.29, 7.99]). Possible benefits from reducing the use of alternative prevention measures (masks, social distancing) and increasing productivity/lowering healthcare costs were rated significantly lower.[3] Still, all benefits were considered, on average, to be important (see Appendix item II).
In comparing various possible concerns about GUV light, respondents felt that the most significant concern was that ‘the technology needs to be tested more before it should be used widely, followed by a concern that this technology might have negative effects on health’ (see Appendix item III).
We also asked respondents how much they would support or oppose the use of GUV light if more research was done and evidence showed it was safe and effective, and separately, if regulators approved this technology. In both situations, levels of support were high, though levels of strong support were higher for the evidence condition.
87.02% of respondents would support GUV light (95% CI [78.9%, 92.3%]) if there were evidence showing it was safe and effective, while 82.33% of respondents said they would support GUV light if regulators approved the technology (95% CI [74.6%, 88.1%]).
Survey 3 had a sample of 2,490 respondents.
We found that respondents receiving the control condition (a more general description of GUV light) showed stronger levels of support than those who received more information about specific types of GUV light systems, e.g., upper-room UVC and far-UVC (see Appendix IV for the text of descriptions).
We also observed more support for general UV light, followed by far-UVC light, followed by upper-room UVC light. This pattern of results was fairly consistent; it was found in all conditions except the control condition.
The inclusion of diagrams did not seem to affect average levels of support in any statistically significant way.
Figure 3: Summary of results of Survey 3, levels of support for GUV under different conditions.
Survey 4 had a sample of 3,508 respondents.
The framings of benefits used in this survey were worded as follows:
If [germicidal light term] light is used in public indoor spaces (e.g., offices, schools, transport hubs, etc.), this will help ensure that alternative prevention measures, such as social distancing, school and restaurant closures, and masking, would not have to be used.
If [germicidal light term] light is used in public indoor spaces (e.g., offices, schools, transport hubs, etc.), this will help ensure that the elderly, young, and vulnerable are protected from infectious diseases.
If [germicidal light term] light is used in public indoor spaces (e.g., offices, schools, transport hubs, etc.), this will help ensure that society-wide pandemics such as COVID-19, or much worse pandemics, would not happen again.
If [germicidal light term] light is used in public indoor spaces (e.g., offices, schools, transport hubs, etc.), this will help ensure that you are protected from infectious disease and are less likely to miss work or a social activity because of illness.
If [germicidal light term] light is used in public indoor spaces (e.g., offices, schools, transport hubs, etc.), this will help ensure that you and those you know are protected from infectious diseases.
There were no significant differences in the level of support for the various framings of the benefits of GUV light when varying between different types of light (see Appendix item V).
Consistent with survey 3, there was more support for germicidal light in general than for far-UVC lights and upper-room UVC lights. Generally, there was more support for far-UVC lights than upper-room UVC lights across the different messages.
Manipulating whether respondents received a description mentioning ‘UV’ explicitly or not, did not have a statistically significant effect on how the messages were perceived (i.e., did not lead to differences in support) (see Appendix item VI).
We did observe an interaction between the framing and the type of light. More support was found for UV lights and far-UVC lights if they were referred to as germicidal light or low-wavelength germicidal light. The opposite was found for upper-room UVC light; more support for this type of light was found when referred to as upper-room UVC light than upper-room germicidal light.
Why examining these results matters
Firstly, as far as we know, there has not been any survey done on US public attitudes towards GUV light as a means of reducing risks from pathogens. However, GUV light represents one of the most promising known technologies for reducing catastrophic biorisk and would likely confer near-termist benefits as well (reduced illness from infectious disease, reduction in ‘sick days’ from workers, etc.) [see this report for more detail]. Understanding public support for and awareness of these technologies, what framings of benefits are most compelling, and what concerns exist should be helpful for developing strategies around advocacy and expanding deployment.
Survey results show moderate awareness of GUV and low awareness of far-UVC (potentially the most effective GUV light technology for reducing catastrophic biorisk). This implies that there is a lot of scope to improve overall awareness of GUV light as a biosecurity measure, for example, through write-ups in reputable news sites and publications.
Despite low levels of awareness, once respondents were provided with a description of the technology, support for GUV light and its subtypes was broadly positive. The support was consistent across multiple surveys and included support for concrete actions such as changing regulations to make it easier to use GUV lights and buying a UVC light for their home.
The results of these surveys seem to confirm and disconfirm intuitions in the biosecurity/indoor air quality community around public attitudes towards GUV technology. These results could be relevant when considering ways to support deploying these technologies to reduce risks from infectious diseases, including pandemics.
As is commonly discussed in indoor air quality circles (based on my experience), safety concerns seem to be a meaningful factor in public perception of this technology. Respondents’ most prominent concern was that GUV lights need additional testing to establish more evidence on safety and efficacy and that the technology would have direct negative effects on health. It should be noted that respondents were not given much information about the current state of the evidence on the safety and efficacy of GUV lights, so it’s difficult to extrapolate from this result to any conclusion about the amount of evidence needed to assuage safety concerns.
Related to the above, we examined whether the public would be more supportive of the technology if research showed it was safe and effective or if regulators approved this technology. Support levels did not seem to differ in the regulatory approval scenario, but in the additional evidence scenario, support was around 87% compared to around 81% from the earlier question gauging general support. There are still reasons we might want to get regulatory support for this technology (e.g., supportive guidelines from the CDC or ASHRAE):
It’s plausible that members of the public, especially office managers or school district officials, use regulatory support as a heuristic for evidence of safety and efficacy.
For far-UVC, it’s likely that dosage limits need to be increased in the US and internationally to maximize the chance of it being used to reduce catastrophic biorisk.
One debate in the indoor air quality community concerns which GUV technology to promote more: upper-room UVC or far-UVC. One position is that since far-UVC involves direct light exposure to humans, people are less likely to support it. This does not seem to be borne out by the survey results, as respondents consistently showed slightly greater support for far-UVC over upper-room UVC. Our interpretation is that this is because, in the description for these technologies, we note that upper-room UVC light can damage eyes and skin (hence they must be installed in the upper part of the room) while we note that far-UVC light ‘may be safer and evidence suggests it has little to no effect on skin or eyes.’ We note, though, that this light ‘has been tested less than other forms of germicidal light.’ Additional testing, using additional frames/descriptions, could tease out the reason behind this result and explore this further.
Another discussion in the indoor air quality community concerns what to call far-UVC. Various names have been proposed, including far-UV, low-wavelength light, and low-wave. One crux in this conversation is the possibility that including UV in the term will prime people to be more concerned about safety, given the associations between UV light and cancer. Our survey shows no statistically significant difference in support when using terms that mention UV vs don’t mention UV.
Possible further investigation
While we have not planned any follow-up surveys on this topic as of the date of publication, there are a few possible avenues that may be worth pursuing in the future.
First, there could be additional surveys that are designed to tease out different explanations for the two counterintuitive findings: (1) relatively more support for far-UVC than upper-room UVC, and (2) the lack of effect on support for these technologies when using terms that include ‘UV’ and terms that don’t. For the former, an additional survey could try to investigate if relative levels of support for far-UVC vs upper-room UVC can be explained largely by the fact that upper-room UVC involves light bands that are harmful if people are directly exposed. We may also want to compare other UVC set-ups such as in-duct UVC, which uses the same wavelength range as upper-room but is more clearly unlikely to come into contact with humans. For the latter, we could see if this finding holds in countries where the association between UV light and skin damage is likely to be stronger, e.g., Australia.
There are also some additional surveys that can be done around testing specific terminology, such as whether referring to these technologies as ‘germicidal ultraviolet light’ vs. ‘ultraviolet germicidal irradiation’ affects support or concerns about safety.
We could also look at public support for these technologies and for different framings of benefits in different countries. Japan and India stand out as two possibilities that might be worth exploring to contrast with existing data about the US and the UK.
There may also be value in gauging support for ‘indoor air quality’ advocacy and messaging more generally since there are other technologies, such as in-room air cleaners and ventilation, that have some role to play in reducing indoor pathogen transmission and catastrophic biorisk. A survey could compare support for ‘indoor air quality’ with other public causes such as cancer or climate change. The case for indoor air quality can be made to the public on the basis of both immediate benefits (reducing air pollution and general infectious illnesses) and for GCBR-related reasons, e.g., reducing risks associated with catastrophic pandemics. Groups planning to push for increased funding and public support for indoor air quality may want to test the appeal of these different framings.
Acknowledgements
This post is a project of Rethink Priorities–a think tank dedicated to informing decisions made by high-impact organizations and funders across various cause areas. It was written by Jam Kraprayoon. Thanks to contributions from David Moss, Jamie Elsey and Willem Sleegers for running the survey, analyzing the results, providing feedback to this write-up, and providing data visualization, as well as Renan Araujo and Linch Zhang for their general advice and support. If you are interested in RP’s work, please visit our research database and subscribe to our newsletter.
- ^
You can learn more about the GUV light and its subtypes here.
- ^
- ^
The possible benefit of GUV light for reducing the use of alternative prevention measures was considered the second least important (M=7.34, 95% CI [6.97, 7.7]), and increasing productivity and lowering healthcare costs was considered the least important (M=7.03, 95% CI [6.73, 7.33].
Appendix
I. How much would you support or oppose the use of germicidal UV light in each kind of place?
| Place | Response | Percentage | 95% CI |
| Hospitals | Oppose | 5.26% | [3.17%, 8.60%] |
| Neither support nor oppose | 12.25% | [9.04%, 16.4%] | |
| Support | 82.49% | [77.8%, 86.3%] | |
| Large crowded public areas | Oppose | 8.99% | [6.00%, 13.3%] |
| Neither support nor oppose | 14.04% | [11.2%, 17.4%] | |
| Support | 76.97% | [72.4%, 81.0%] | |
| Private areas of businesses | Oppose | 8.07% | [5.18%, 12.4%] |
| Neither support nor oppose | 13.63% | [10.8%, 17.1%] | |
| Support | 78.30% | [73.7%, 82.3%] | |
| Public areas of businesses | Oppose | 6.86% | [4.62%, 10.1%] |
| Neither support nor oppose | 13.84% | [10.6%, 17.9%] | |
| Support | 79.30% | [74.8%, 83.2%] | |
| Schools | Oppose | 12.27% | [8.58%, 17.2%] |
| Neither support nor oppose | 12.04% | [9.35%, 15.4%] | |
| Support | 75.70% | [70.7%, 80.1%] | |
| Transport hubs | Oppose | 7.28% | [4.60%, 11.3%] |
| Neither support nor oppose | 11.07% | [8.49%, 14.3%] | |
| Support | 81.66% | [77.2%, 85.4%] |
II. Possible benefits of germicidal UV light
| Benefit | M | 95% CI |
| Reduce risk of getting sick | 7.47 | [7.13, 7.81] |
| Reduce risk for vulnerable people | 7.64 | [7.29, 7.99] |
| Reduce risk of society-wide pandemics | 7.51 | [7.18, 7.84] |
| Reduce the use of alternative prevention measures | 7.34 | [6.97, 7.7] |
| Increase productivity and lower healthcare costs | 7.03 | [6.73, 7.33] |
III. Possible concerns about germicidal UV light
Please consider the following possible concerns about this technology:
The technology needs to be tested more before it should be used more widely
If this is installed in public areas, individuals will not have a choice about whether or not they enter locations using this technology
I do not believe this technology is safe
I have heard that UV light is dangerous, and so I am concerned about negative effects
Even if this technology is safe when installed properly, I worry that sometimes people will make mistakes when installing it and it will be unsafe
I do not believe this technology will work effectively to reduce illness
There may be indirect negative effects from reducing our exposure to pathogens (e.g., reducing our immunity to these diseases)
If governments decide to subsidize this, it may cause a rise in taxes
If governments make this a requirement, the additional cost for business owners may lead to a rise in prices
| Concern | M | 95% CI |
| Needs to be tested more | 7.46 | [7.19, 7.73] |
| People will not have a choice | 6.35 | [6, 6.7] |
| Might not be safe | 6.91 | [6.59, 7.23] |
| Negative effects | 7.01 | [6.69, 7.33] |
| People might make mistakes when installing it | 6.25 | [5.86, 6.64] |
| Might not work effectively | 6.71 | [6.38, 7.03] |
| There may be indirect negative effects | 6.67 | [6.34, 7] |
IV. Descriptions of GUV light systems
Control
Scientific research has shown that germicidal UV light can be used to destroy or disrupt germs such as bacteria and viruses, reducing their spread. Such germicidal UV light can be used in buildings – such as workplaces, hospitals, homes, or schools – to kill viruses and bacteria in the air. This then lowers the chances of people in these buildings becoming sick. This could work for existing illnesses, such as colds and flu and COVID-19, and could also reduce the risk from new or even engineered viruses.
Some types of germicidal UV light can be harmful to the eyes or skin if people are directly exposed to them. If this kind of light were used in buildings, it would need to be set up in ways that did not directly expose humans to the light, but would still clean germs in the air (e.g., through installing the lights in air ducts, or in the upper part of a room (called upper room UVC), where they clean circulating air). Another type of germicidal UV light (called low-wavelength light or far-UVC), may be safer. It has little to no effects on the skin or eyes, while still killing germs.
Explicit germicidal + far UV + no diagram
Scientific research has shown that germicidal UV light can be used to destroy or disrupt germs such as bacteria and viruses, reducing their spread. Such germicidal UV light can be used in buildings – such as workplaces, hospitals, homes, or schools – to kill viruses and bacteria. This then lowers the chances of people in these buildings becoming sick. This could work for existing illnesses, such as colds and flu and COVID-19, and could also reduce the risk from new or even engineered viruses.
One method of using germicidal UV light to reduce the spread of pathogen transmission in buildings is to install the lights where they can disinfect the air, for example in air ducts, or by positioning the light near the ceiling (called upper-room UV), so that it can disinfect air as it circulates to the top of the room. This form of germicidal UV light can damage human skin and eyes, so it is important that they are properly installed in the upper part of the room to prevent direct contact with people in the room.
Another form of germicidal light is called far-UVC. This form of light may be safer, and evidence suggests that it has little or no effect on the skin or eyes, while still killing germs. However, it has been tested less than other forms of germicidal light. This form of germicidal light could be shone throughout rooms, meaning that it could disinfect air throughout the room and on surfaces, though also meaning that it would be in contact with the skin of people in the room.
Explicit upper-room condition + diagram
Scientific research has shown that germicidal UV light can be used to destroy or disrupt germs such as bacteria and viruses, reducing their spread. Such germicidal UV light can be used in buildings – such as workplaces, hospitals, homes, or schools – to kill viruses and bacteria in the air. This then lowers the chances of people in these buildings becoming sick. This could work for existing illnesses, such as colds and flu and COVID-19, and could also reduce the risk from new or even engineered viruses.
One method of using germicidal UV light is called upper room UVC. With this method, the spread of pathogen transmission in buildings can be reduced by installing the lights where they can disinfect the air by positioning the light near the ceiling, so that it can disinfect air as it circulates to the top of the room. This form of germicidal UV light can damage human skin and eyes, so it is important that they are properly installed in the upper part of the room to prevent direct contact with people in the room.
Another form of germicidal light is called far-UVC. This form of light may be safer, and evidence suggests that it has little or no effect on the skin or eyes, while still killing germs. However, it has been tested less than other forms of germicidal light. This form of germicidal light could be shone throughout rooms, meaning that it could disinfect air throughout the room and on surfaces, though also meaning that it would be in contact with the skin of people in the room.
Explicit low wavelength
Scientific research has shown that germicidal light can be used to destroy or disrupt germs such as bacteria and viruses, reducing their spread. Such germicidal light can be used in buildings – such as workplaces, hospitals, homes, or schools – to kill viruses and bacteria. This then lowers the chances of people in these buildings becoming sick. This could work for existing illnesses, such as colds and flu and COVID-19, and could also reduce the risk from new or even engineered viruses.
One method of using germicidal light to reduce the spread of pathogen transmission in buildings is to install the lights where they can disinfect the air, for example in air ducts, or by positioning the light near the ceiling (called upper room germicidal light), so that it can disinfect air as it circulates to the top of the room. This form of germicidal light can damage human skin and eyes, so it is important that they are properly installed in the upper part of the room to prevent direct contact with people in the room.
Another form of germicidal light is called low wavelength light. This form of light may be safer and evidence suggests that it has little or no effect on the skin or eyes, while still killing germs. However, it has been tested less than other forms of germicidal light. This form of germicidal light could be shone throughout rooms, meaning that it could disinfect air throughout the room and on surfaces, though also meaning that it would be in contact with the skin of people in the room.
Explicit low wavelength + upper-room condition + diagram
Scientific research has shown that germicidal light can be used to destroy or disrupt germs such as bacteria and viruses, reducing their spread. Such germicidal light can be used in buildings – such as workplaces, hospitals, homes, or schools – to kill viruses and bacteria in the air. This then lowers the chances of people in these buildings becoming sick. This could work for existing illnesses, such as colds and flu and COVID-19, and could also reduce the risk from new or even engineered viruses.
One method of using germicidal light is called upper room germicidal light. With this method, the spread of pathogen transmission in buildings can be reduced by installing the lights where they can disinfect the air by positioning the light near the ceiling, so that it can disinfect air as it circulates to the top of the room. This form of germicidal light can damage human skin and eyes, so it is important that they are properly installed in the upper part of the room to prevent direct contact with people in the room.
Another form of germicidal light is called low wavelength light. This form of light may be safer and evidence suggests that it has little or no effect on the skin or eyes, while still killing germs. However, it has been tested less than other forms of germicidal light. This form of germicidal light could be shone throughout rooms, meaning that it could disinfect air throughout the room and on surfaces, though also meaning that it would be in contact with the skin of people in the room.
V. Message testing
| Condition | Light type | Support | 95% CI |
| alternative prevention measures | UV lights | 5.32 | [5.21, 5.44] |
| far-UVC lights | 5.20 | [5.08, 5.31] | |
| upper-room UVC lights | 5.14 | [5.02, 5.26] | |
| elderly, young, and vulnerable | UV lights | 5.43 | [5.31, 5.54] |
| far-UVC lights | 5.26 | [5.14, 5.37] | |
| upper-room UVC lights | 5.21 | [5.1, 5.33] | |
| society-wide pandemics | UV lights | 5.46 | [5.34, 5.58] |
| far-UVC lights | 5.32 | [5.2, 5.44] | |
| upper-room UVC lights | 5.24 | [5.13, 5.36] | |
| work or a social activity | UV lights | 5.38 | [5.26, 5.5] |
VI. Mentioning ‘UV’ vs. not mentioning ‘UV’
| Condition | Light type | Support | 95% CI |
| UV lights | germicidal light | 5.43 | [5.35, 5.5] |
| UV | 5.34 | [5.26, 5.41] | |
| far-UVC lights | germicidal light | 5.27 | [5.2, 5.34] |
| UV | 5.16 | [5.09, 5.24] | |
| upper-room UVC lights | germicidal light | 5.14 | [5.07, 5.21] |
| UV | 5.19 | [5.12, 5.26] |
There was a significant interaction effect between condition and which term was used to describe the UV light (i.e., light type), F(2, 5996) = 7.26, p < .001). Inspecting the effect of the framing for each condition separately shows that there is no effect of framing in the UV lights and upper-room UVC lights condition, but there is a just significant result in the far-UVC lights condition.
| Condition | b | SE | df | t | p |
| UV lights | 0.09 | 0.05 | 4,938.48 | 1.68 | .092 |
| far-UVC lights | 0.11 | 0.05 | 4,938.48 | 1.99 | .046 |
| upper-room UVC lights | −0.05 | 0.05 | 4,938.48 | −0.95 | .34 |
- Thoughts on far-UVC after working in the field for 8 months by (31 Jul 2023 14:36 UTC; 234 points)
- 20 concrete projects for reducing existential risk by (21 Jun 2023 15:54 UTC; 132 points)
- EA Organization Updates: February 2023 by (14 Feb 2023 21:39 UTC; 43 points)
- EA & LW Forum Weekly Summary (30th Jan − 5th Feb 2023) by (7 Feb 2023 2:13 UTC; 21 points)
- 's comment on Donation recommendations for xrisk + ai safety by (8 Feb 2023 14:03 UTC; 4 points)
- EA & LW Forum Weekly Summary (30th Jan − 5th Feb 2023) by (LessWrong; 7 Feb 2023 2:13 UTC; 3 points)
Thanks for running the survey and writing up what you found! I’ve shared this with other people who are also looking into UV.
Regarding “Mentioning ‘UV’ vs. not mentioning ‘UV’”, what terminology was used in the “not mentioning UV” condition?
We used the following terms:
Germicidal light vs. Germicidal UV light
Low wavelength light vs. Far-UVC
Upper room germicidal light vs. upper room UVC
This and their accompanying descriptions (which were otherwise kept the same) can be found in Appendix item IV, ‘Description of GUV light systems’.