How a ventilation revolution could help mitigate the impacts of air pollution and airborne pathogens
edited By Adam Thompson and Joe Buckley
This is a repost from a policy report I wrote a few months back for the UK Labour party here
In searching for air pollution on EA forum, I just came across and read this nice article, which goes into the specifics of the cost effectiveness of using air purifiers to mitigate PM2.5. Otherwise I didn’t see many articles on the EA forum on this topic, despite its considerable public health impact. Furthermore, mitigation strategies suggested here would also increase our resilience to future pandemics & airborne bio risks.
Summary
Governments across the world have made considerable efforts to legislate for food safety, sanitation and drinking water for public health purposes. However, little attention has been given to the quality of air we breathe. Much of the focus around air pollution in recent years has been on outdoor air pollution, but recent studies suggest indoor air pollution can be many times worse, and yet it remains poorly monitored and mitigated.
Air pollution in the major UK cities has been found to be significantly above legal and recommended levels, and is a major cause of lung disease, stroke and heart disease, and has been linked to increases in child asthma, obesity, mental health issues, and COVID-19 mortality. Recently, a nine year old (Ella Adoo-Kissi-Debrah) was the first person in the UK to have air pollution listed as a cause of death, though it is estimated that 40,000 premature deaths in the UK result each year (~8% of all deaths). Evidence shows that in the developed world, we spend up to 90% of our time indoors, yet concentrations of some pollutants can be 2 to 5 times higher than outdoors.
Our policy recommendations include, (i) reducing the source of contaminants (indoor and outdoor, (ii) implementing monitoring and enforce safe indoor limits for pollutants and degree of recirculated air (via CO2); and (iii) installing better ventilation and filtration systems in schools, offices and public buildings. Implementing these would not only help improve the consequences arising from air pollution, but also be transformative in controlling and limiting the spread of respiratory viruses such as COVID-19, flu and other airborne pathogens. Technology already exists to monitor, disinfect and filter air, yet because of weak air quality building regulations, architects and building engineers have instead focussed on thermal comfort, odour control and energy use, whilst neglecting infection control.
Installing or retrofitting ventilation and filtration systems in our buildings will have a cost, but in doing so, it will reduce economic losses from air pollution and respiratory viruses as a result of sick leave and NHS-related health costs. The cost of COVID-19 to the UK in 2020 has been estimated at £251 billion, while, each year, air pollution costs the UK £54 billion, seasonal influenza £30 billion and other respiratory infections £11 billion.
At a critical time in the COVID-19 pandemic, with the environmental bill returning to parliament this autumn and looking to the future, a ventilation revolution may reduce preventable health and economic suffering from both air pollution and airborne illnesses simultaneously.
Introduction
There is now overwhelming and increasing scientific evidence from thousands of studies, that air pollution (both indoor and outdoor) is a significant problem for human health (Schraufnagel et al., 2019). The World Health Organisation (WHO) calls air pollution the world’s largest single environmental health risk. With 90% of the world living in areas above the WHO air pollution limit, air pollution is the 4th highest cause of worldwide deaths, accounting for 5 million premature deaths each year (Ritchie and Roser, 2017). Despite this, compared to food safety, drinking water contamination and hand washing hygiene, air quality is far less regulated and invested in (Morawska et al., 2021).
Air pollution has been called ‘the invisible killer’, not only as we are unable to see it, but also because of its effects on human health, which often occur on longer timescales (years or decades), producing chronic health effects that look similar to other diseases (such as heart attacks) (Fuller, 2018). Scientists have been able to associate air pollution with premature deaths using large correlative datasets correcting for other factors and also by studying the direct effects on human organs and cells (Ritchie and Roser, 2017).
In the UK, air pollution levels in UK have gradually been decreasing, however Public Health England (PHE) maintains that air pollution is the biggest environmental threat to health in the UK, suggesting that there could be ~2.5 million new cases of coronary heart disease, stroke, lung cancer, childhood asthma, chronic obstructive pulmonary disease, diabetes, low birth weight and dementia by 2035 if current air pollution levels persist (PHE, 2018). In the UK, two thirds of the population are exposed to air pollution above the WHO legal limit for particlulate matter that is 2.5 micrometres or less in diameter (PM2.5) (Ritchie and Roser, 2017). In addition, nitrogen dioxide (NO2) levels have been illegally high in most urban areas since 2010 with the government having lost three times in court over the adequacy of its plans to reduce pollution levels (The Guardian, 2021).
The UK has one of the highest percentage of deaths from air pollution in the G7 (see figure 1). Considering the recent estimate from the Royal College of Physicians of 40,000 deaths, these data may be an underestimate, instead values for the UK may be up to an 8% share of deaths in the UK, at a rate of 59 deaths per 100,000 (Royal College of Physicians, 2016).
Air pollution and respiratory viruses such as SARS-COV-2 are not independent from each other, with recent studies showing that small increases in air pollution (predominantly NO2 and PM2.5) leads to a large increase in the COVID-19 infectivity and mortality rate in England (Travaglio et al., 2021).
Here, we assess the extent of the health and economic problems associated with air pollution and airborne viruses (such as COVID-19) and how their effects may be minimised effectively and quickly by implementing regulations to monitor and ventilate indoor spaces.
Outdoor and indoor air pollution
What is it and where does it come from?
Air pollution conventionally applies to both the small particles and gases emitted from industries (e.g. coal burning), transport (both combustible emissions and tyre & brake debris), home heating and agriculture. These pollutants include gases such as nitrogen dioxide, ammonia, ozone, sulphur dioxide and carbon monoxide, particulate matter made up of solid and liquid particles such as soot and dust of various sizes (PM10, PM2.5). These pollutants are distinct from the human-made gases that lead to atmospheric warming such as carbon dioxide and methane. Although air pollution has generally improved in recent decades in Europe, as the effects of climate change increase, smoke and particulate matter from forest fires, soil erosion and increased desertification can travel thousands of kilometres and affect air pollution in the UK (e.g. Russian wildfires: (Witham and Manning, 2007)).
The worst health effects seem to be associated with fine particulate matter (PM2.5), nitrogen dioxide (emitted from diesel) and ozone. These outdoor pollutants can become concentrated indoors up to 2 to 5 times, especially in poorly ventilated areas (Environmental Protection Agency, 2021). For example, PM2.5 levels within the London underground were found to be 4 times higher than roadside environments in central London, and 30 times higher than the WHO recommended limits (Smith et al., 2020). Additionally, nitrogen dioxide levels (emitted from diesel train engines) within UK railway stations (e.g. Birmingham New Street) were up to 8 times higher than outdoor EU limits (Hickman et al., 2018).
Not only do indoor settings concentrate outdoor pollution, but further sources of pollutants are found indoors and even in our homes, from wood burning stoves, boilers, building materials such as types of wood and plaster, smoking, household products, and the use of un-vented, fuel-burning appliances like gas stoves or kerosene space heaters. These sources can introduce harmful pollutants in the form of volatile organic compounds (VOCs) such as benzene and formaldehyde, as well as carbon monoxide, radon, and fine particulate matter (PM2.5).
Air pollution effects on human health
Air pollution has now been show to affect every organ and cell in the body, and black carbon particles have been found to pass through the placental barrier (the Guardian, 2019; Schraufnagel et al. 2019). The most common problems relate to respiratory, pulmonary disease and cardiovascular inflammation leading to lung and heart disease. However, air pollution has also been linked with a wide range of conditions such as depression, cancer, reduced fertility, increased miscarriages, Alzheimer’s disease, strokes, diabetes and reduced intelligence (Schraufnagel et al., 2019). Worryingly, children in the most polluted parts of London are growing smaller lungs, with dirty air linked to mental health issues, obesity and increased respiratory illnesses (Mudway et al., 2019). Air pollution is also known to exacerbate pre-existing (mostly respiratory) illnesses, such as asthma, which 1.1 million UK children suffer from, with a quarter of UK pupils (3.4 million) attending schools where air pollution is worse than the WHO limit (The Guardian, 2021). Not only does air pollution account for millions of premature deaths, but it is one of the main contributors to disease burden (the number of years lived in poor health), thus negatively affecting quality of life (Ritchie and Roser, 2017).
Exposure to poor air quality is generally higher in the most deprived areas in the UK, affecting those living closer to roads and in highly populated urban areas, suggesting that the worst health effects are felt by the most vulnerable, intensifying inequalities (Brunt et al., 2017). One tragic example is death of Ella Adoo-Kissi-Debrah (aged 9), who lived beside the South Circular in London and was the first person in the UK to have air pollution officially listed on her death certificate (BBC, 2021).
Airborne viruses and pathogens
An extra incentive to solve the air quality problem is the widespread presence of COVID-19 and other respiratory illnesses, which have provided a heighted awareness about how contaminated the air that we breathe is. At the beginning of the pandemic, it was not expected that SARS-COV-2 virus was spread via airborne transmission, with much of the measures to tackle the virus in UK based around hand washing and the 2-metre rule, as it was thought that transmission occurred via surface contamination and via droplets (particles > 5 micrometres). But, since October 2020, scientific consensus confirmed that COVID-19 was mainly spread by aerosol transmission (particles < 5 micrometres) (Morawska and Cao, 2020). Despite knowing of COVID-19’s airborne transmission for almost a year, including the type of activities that produce the most airborne transmission, and how air flow moves particles in enclosed spaces, the UK government has made little progress on mitigating airborne transmission. As well as COVID-19, many other pathogens are spread via airborne transmission, such as the common cold, flu, TB, measles, SARS and norovirus. Therefore, stricter indoor air quality controls will also lower the human and economic suffering from annual flu and other common viruses. The combined economic costs from employee sick leave and direct use of the NHS from COVID-19, flu and air pollution have a substantial economic cost each year (see figure 2), particularly when compared to other costs that the UK spends sizable time and money to mitigate the effects of, such as smoking, alcohol and obesity. The UK government must act to limit the effects of air pollution and airborne diseases. Below, we suggest several, tractable ways in which these can be tackled simultaneously.
Policy suggestions
We suggest three ways of mitigating the effects from both air pollution and airborne viruses:
Tackle the source of contaminants (indoor and outdoor);
Implement monitoring and enforce safe indoor limits for pollutants and degree of recirculated air (via CO2); and
Install effective filtration and ventilation systems to minimise pathogens and pollutants.
Tackle the source of contaminants (indoor and outdoor)
One of the first steps to improve air quality would be for the UK to adopt the WHO limits for air pollution, which are 2.5 times lower than the UK’s limits for PM2.5, something that was advised by the coroner of Ella Kiss-Debra (BBC, 2021). The environmental bill this autumn provides an opportunity to do this and to redesign our pollution laws for the 21st century.
Generally, air pollution in the UK has improved in the last few decades, with fewer diesel and more efficient vehicles, burning of ‘cleaner’ fossil fuels and effective regulation at the UK and European level since the 1970s (Carnell et al., 2019). More recent efforts, such as the introduction of low emission zones can be effective, particularly for NO2 levels, however, seem to have less of an effect on PM2.5 and PM10 (Mudway et al., 2019). This fact, and the higher death share from pollution compared to others in the G7 (see figure 1), suggest that these measures are currently insufficient to mitigate the widespread effects on public health. The lack of progress on this front is in part a political problem, whereby central government is reluctant to impose ultra-low emission zones (more effective solutions than low emission zones) as they can be seen as unpopular. These responsibilities are instead pushed to local councils, who generally have neither the resources or the knowhow to implement such schemes.
Other policy suggestions include:
Further taxes on the big polluters, such as fossil fuel companies, diesel vehicles, wood burning households and on VOC-rich building materials
These are some of the largest sources of PM2.5 and NO2 and taxes may discourage their use or encourage innovations to make them cleaner (e.g. scrubbing or filtering of gases/particulate matter). It may also provide an extra source of income monitor and enforce ultra-low emission zones and the other suggestions below.
Campaigns to crackdown on engine idling near schools or other urban areas
An idling engine can produce up to twice as many exhaust emissions as an engine in motion and as a consequence is against the law, with a fixed penalty of £20. Despite this, there is little awareness of this harm this may cause especially when parked near schools, nurseries or other vulnerable adults.
Better city planning to support cycling and walking.
This measure may require extra financial assistance from the UK government, but it would benefit personal health and fitness, urban air quality and help to minimise our carbon footprint.
Actions to limit outdoor air pollutants may lower COVID-19 mortality (Travaglio et al., 2021), whilst also reducing our carbon emissions, helping to meet our net zero goals as we prepare for COP26.
2. Implement monitoring and enforce safe indoor limits for pollutants and degree of recirculated air (via CO2 monitors)
Current regulations around indoor air quality are lacking, and while some guidelines and concentration limits from the WHO do exist (WHO, 2010), they are rarely enforced in our workplaces, transport systems, homes, cars, schools, nurseries, shops and restaurants. Indoor air quality may be especially in poor in areas where outdoor air pollution is high, after recent renovations and in poorly ventilated and poorly insulated buildings.
Monitors to measure harmful pollutants such as PM2.5, NO2, formaldehyde and other VOCs, can be found on the market and are relatively inexpensive. By routinely measuring these pollutants via regular visits to public indoor spaces and comparing these to ‘safe limits’ defined by the WHO, we may begin to understand the extent of the problem and, if required, further steps can be taken to mitigate this problem, such as mechanical and or natural ventilation.
Measuring the degree of recycled air is a critical component for mitigating the effects of airborne transmission of pathogens such as SARS-COV-2. This degree can approximated using CO2 monitors (HSE 2021). The atmosphere contains ~400 ppm CO2, and humans breathe out ~40,000 ppm CO2, therefore a measurement of 4000 ppm suggests that 10% of the air is recycled. Measures to lower this value as much as possible through natural or mechanical ventilation will limit the spread of airborne pathogens such as SARS-COV-2. Non-dispersive infrared CO2 monitors are cheap (£150), the technology is readily available, and can be implemented immediately. CO2 monitoring could, therefore, be instrumental in the fight against COVID-19 and other viruses.
In high enough concentrations or in a small or poorly ventilated space, CO2 (from human exhalation) can also cause harmful effects, and is linked to a disorder commonly referred to as ‘sick building syndrome’, which is associated with headaches, tiredness, shortness of breath (Apte, Fis and Daisey, 2000). CO2 concentration is something taken more seriously in other countries, such as Germany, where CO2 monitors and awareness of air quality in general are commonplace. Encouragingly, the use of CO2 monitors to monitor the extent of recirculated air has recently been put forward by unions and medical organisations for schools, in the fight to reduce COVID-19 cases (BBC, 2021), but this information itself may not solve the problem and further actions need to be employed (see table 1). For example, in rooms without windows or sources of fresh air, mechanical ventilation and filtration may be necessary. If we are to keep COVID-19 cases down this autumn and winter as millions return to work, more widespread CO2 monitoring could and should be required.
Table 1. Costs associated with action to improve indoor air quality and contamination
| Action | Cost |
| Opening windows; inspecting and maintaining dedicated exhaust ventilation; repositioning outdoor air dampers | No cost |
| Using fans to increase effectiveness of open windows; repositioning supply/exhaust diffusers to create directional airflow | Less than £100 |
| Monitors to measure recycled air/ventilation via CO2, as well as air pollutants formaldehyde, PM2.5, NO2. | Approximately £500 |
| Adding portable HEPA fan/filter and/or ultra-violet purification systems | £500 to £4000 (depending on room size): |
3. Installation of effective filtration and ventilation systems
One of the best ways of mitigating the indoor air pollution problem is to make buildings airtight and install ventilation systems that reduce the inflow of outdoor pollutants, while preventing the build-up of indoor pollutants. Current ventilation building regulations are lacking and are used mostly to remove odours, or to cool or heat air (Morawska et al., 2021).
Effective filtration and disinfection technology already exists both for the domestic environment (Dyson Air Purifier, Blueair) and well as the commercial (Rensair) (see figure 3) which trap particles as low as 0.1 micrometres in size, using high-efficiency particulate absorbing (HEPA) and carbon filters.
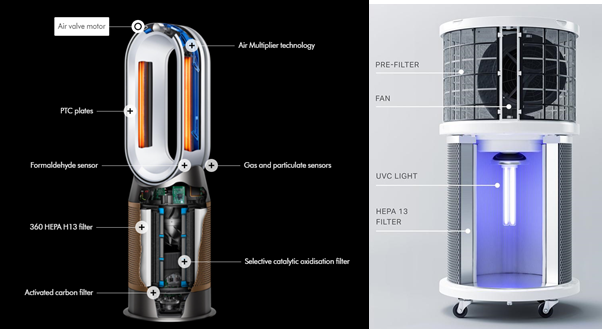
Effective filtration is, therefore, able to capture the vast proportion (> 99%) of harmful gases, particulate matter and pathogens, as shown in laboratory tests (Danish Institute of Technology, 2021). Technologies exist to not only filter, but also disinfect the air using ultra-violet light removes 99% of airborne viruses and bacteria, including 99.99 of airborne SARS-COV-2 in lab conditions (see figure 3) (Danish Institute of technology, 2021). However, mechanical ventilation must be implemented effectively to ensure it does not recirculate and filtrate the indoor air, as in some air conditioning units. Ideally, mechanical ventilation systems should draw in filtrated outdoor air, perhaps utilising existing air flow systems with the extent of recycled air monitored using CO2 monitors and the harmful pollutants using PM2.5, NO2 and VOC monitors.
Conclusions
Air pollution has a significant health and economic impact to the UK population. Mitigation efforts have, so far, concentrated on tackling the sources of outdoor pollution, which have improved air quality. However, progress is too slow, with the UK still lagging behind other developed countries, using various metrics. More neglected are regulations to minimise indoor air pollution, where we spend the vast majority of our time, and where more pollution sources exist. Indoor air quality can be improved using inexpensive monitoring of pollutants, and the degree of recycled air using CO2 monitors. Setting safe levels of these pollutants in public places such as classrooms, workplaces, nurseries, hospitals, transport systems and shops, will not only help limit the spread of COVID-19 and other viruses, but also help protect the most vulnerable in society (such as children) from air pollution effects. These measures, along with effective ventilation, filtration and ultra-violet disinfection, can capture particles as small as 0.1 micrometres, lowering levels of harmful particulate matter, gases and also airborne viruses such as COVID-19, flu and the common cold. The beneficial health effects this may have on UK population, as we learn to live with COVID-19, could be significant, as could the effects of preventing economic losses from sick days and strain on the NHS.
Questions for government
We recommend the following questions are posed to the Government in the run-up to COP26:
What is the case for not lowering UK air pollution limits to WHO standards, when the potential economic and health impacts are so large?
How effective is the decentralised approach for reducing outdoor air pollution (i.e. tools such as low emission zones)?
What actions are DEFRA/the government doing to monitor and improve indoor air pollution in public indoor places, such as stations, schools, hospitals, and the hospitality sector?
When will the government to reduce its NO2 and PM2.5 levels to legal limits, and how will that reduction be achieved?
Has the government performed a cost benefit assessment for the implementation of effective monitoring, filtration and ventilation, to mitigate the effects from COVID-19 and air pollution, versus the costs of doing not taking this action?
References
Alcohol Health Alliance (2020) Written evidence submitted by the Alcohol Health Alliance UK (AHA) (PEG0228). Available at: https://committees.parliament.uk/writtenevidence/10681/pdf/ (Accessed: 4 September 2021).
MG Apte, WJ Fisk and JM Daisey (2000) Associations between indoor CO2 concentrations and sick building syndrome symptoms in U.S. office buildings: an analysis of the 1994-1996 BASE study data. Indoor Air 10 246–257.
BBC (2021) Air pollution: Coroner calls for law change after Ella Adoo-Kissi-Debrah’s death. Available at: https://www.bbc.co.uk/news/uk-england-london-56801794 (Accessed: 2 September 2021).
BBC (2021) Covid: CO2 monitors pledged to aid school ventilation. Available at: https://www.bbc.co.uk/news/education-58285359 (Accessed: 2 September 2021).
Blueair Why Blueair—Performance. Available at: https://www.blueair.com/gb/blueair-performance.html (Accessed: 2 September 2021).
H Brunt, et al. (2017) Air pollution, deprivation and health: understanding relationships to add value to local air quality management policy and practice in Wales, UK. J. Public Health (Oxf.). 39 485–497.
TK Burki (2017) The economic cost of respiratory disease in the UK. Lancet Respir. Med. 5 381.
E Carnell, et al. (2019) Modelling public health improvements as a result of air pollution control policies in the UK over four decades—1970 to 2010. Environ. Res. Lett. 14 074001.
CEBR (2021) One year since lockdown: The £251 billion cost to the UK economy. Available at: https://cebr.com/reports/one-year-since-lockdown-the-251-billion-cost-to-the-uk-economy/ (Accessed: 2 September 2021).
Centre for Mental Health (2017) Mental health problems at work cost UK economy £34.9bn last year, says Centre for Mental Health. Available at: https://www.centreformentalhealth.org.uk/news/mental-health-problems-work-cost-uk-economy-ps349bn-last-year-says-centre-mental-health (Accessed: 2 September 2021).
Dyson Overview | Dyson Purifier Hot + Cool Formaldehyde. Available at: https://www.dyson.co.uk/air-treatment/purifiers/dyson-purifier-hot-cool-formaldehyde/dyson-purifier-hot-cool-formaldehyde-overview (Accessed: 2 September 2021).
Environmental Protection Agency (2021) Indoor Air Quality. Available at: https://www.epa.gov/report-environment/indoor-air-quality (Accessed: 2 September 2021).
G Fuller (2018) The invisible killer: the rising global threat of air pollution: and how we can fight back. (Melville House UK: UK) p. 304.
A Hickman, et al. (2018) Evaluation of air quality at the Birmingham New Street railway station. Proc. Inst. Mech. Eng. F: J. Rail Rapid Transit. 232 1864–1878.
Health and Safety Executive (2021) Identifying poorly ventilated areas and using CO2 monitors. Available at: https://www.hse.gov.uk/coronavirus/equipment-and-machinery/air-conditioning-and-ventilation/identifying-poorly-ventilated-areas.htm (Accessed: 2 September 2021).
International Longevity Centre (2021) Up in smoke: The impact of smoking on health and economic activity. Available at: https://ilcuk.org.uk/up-in-smoke/ (Accessed: 2 September 2021).
International Longevity Centre (2019) Flu costs £30bn in sick days every year, finds new report. Available at: https://ilcuk.org.uk/flu-costs-30bn-in-sick-days-every-year-finds-new-report/ (Accessed: 2 September 2021).
L Morawska, et al. (2021) A paradigm shift to combat indoor respiratory infection. Science. 372 689–691.
L Morawska and J Cao. (2020) Airborne transmission of SARS-CoV-2: The world should face the reality. Environ. Int. 139 105730.
IS Mudway, et al. (2019) Impact of London’s low emission zone on air quality and children’s respiratory health: a sequential annual cross-sectional study Lancet Public Health. 4 e28–e40.
Public Health England (2010) Air pollution: a tool to estimate healthcare costs. Available at: https://www.gov.uk/government/publications/air-pollution-a-tool-to-estimate-healthcare-costs (Accessed: 2 September 2021).
Public Health England (2017) Health matters: obesity and the food environment. Available at: https://www.gov.uk/government/publications/health-matters-obesity-and-the-food-environment/health-matters-obesity-and-the-food-environment--2 (Accessed: 2 September 2021).
Rensair and Danish Institute of Technology (2021) Technology. Available at: https://rensair.com/technology-2/ (Accessed: 2 September 2021).
Royal College of Physicians (2016) Every breath we take: the lifelong impact of air pollution. Available at: https://www.rcplondon.ac.uk/projects/outputs/every-breath-we-take-lifelong-impact-air-pollution (Accessed: 2 September 2021).
H Ritchie and M Roser (2017) Air Pollution. Available at: https://ourworldindata.org/air-pollution (Accessed: 2 September 2021).
DE Schraufnagel, et al. (2019) Air pollution and noncommunicable diseases: a review by the forum of international respiratory societies’ environmental committee, part 1: the damaging effects of air pollution. Chest 155 409–416.
JD Smith, et al. (2020) PM2.5 on the London. Environ. Int. 134 105188.
The Guardian (2021) UK has broken air pollution limits for a decade, EU court finds. Available at: https://www.theguardian.com/environment/2021/mar/04/uk-has-broken-air-pollution-limits-for-a-decade-eu-court-finds (Accessed: 2 September 2021).
The Guardian (2019) Revealed: air pollution may be damaging ‘every organ in the body’. Available at: https://www.theguardian.com/environment/ng-interactive/2019/may/17/air-pollution-may-be-damaging-every-organ-and-cell-in-the-body-finds-global-review (Accessed: 2 September 2021).
The Guardian (2019) Quarter of UK pupils attend schools where air pollution is over WHO limit. Available at: https://www.theguardian.com/environment/2021/jun/17/quarter-of-uk-pupils-attend-schools-where-air-pollution-is-over-who-limit (Accessed: 2 September 2021).
M Travaglio, et al. (2021) Links between air pollution and COVID-19 in England. Environ. Pollut. 268 115859.
World Health Organisation (2010) WHO guidelines for indoor air quality. Available at: https://www.euro.who.int/__data/assets/pdf_file/0009/128169/e94535.pdf (Accessed: 2 September 2021).
World Health Organization Regional Office for Europe (2010) Economic cost of deaths from air pollution (outdoor and indoor) per country, as a percentage of GDP. Available at: https://www.euro.who.int/en/media-centre/sections/press-releases/2015/04/air-pollution-costs-european-economies-us$-1.6-trillion-a-year-in-diseases-and-deaths,-new-who-study-says (Accessed: 4 September 2021).
C Witham and A Manning (2007) Impacts of Russian biomass burning on UK air quality. Atmos. Environ. 41 8075–8090.
Quite timely—I’ve just noticed the first peer-reviewed ‘real-life’ study showing that air filters (HEPA) used in Covid wards in one hospital significantly reduced the presence of airborne SARS-CoV-2: Press-release: https://www.cam.ac.uk/research/news/air-filter-significantly-reduces-presence-of-airborne-sars-cov-2-in-covid-19-wards
Paper: https://academic.oup.com/cid/advance-article/doi/10.1093/cid/ciab933/6414657?guestAccessKey=248e14cc-d920-4782-99b7-634e47cdaa0e
(For context: In the UK more than 11,000 people were thought to have died from catching COVID at hospitals).
Awesome!
It should score high in ITN evaluations. It’s the sort of neglected near-term cause area that can be well understood by normies, could suscite bipartisan support, and so be tackled with more research, inovation and political will. And yet there’s not much material in EA-like sources on that (except for this 80kh interview).
… And I didn’t even know WHO had finally updated its air pollution limits!
Also, sorry if this is stupid, but it seems that, unlike CO2, risks from many pollutants (like particulate matters and pathogens) could be significantly mitigated by effective dispersion; so even a normal ventilator could have observable effect on indoor air quality, right? Thus, I wonder if there are / could be any relevant policy recommendations along this line—like for urban design, e.g., “locate potential air pollution emissions by the sea, or spread through areas where they can be dispersed by winds”. Does it make any sense?
Thanks Ramiro, I hadn’t listened to that 80kh interview-so I’ll do that! But yes it could fall into both ‘Global health and well being’, but also longtermism categories (bio-risk mitigation-wise).
Yes you’re right. I guess there’s a difference between ventilation (dispersing the air around, either ‘natural’ - e.g. windows, or ‘mechanical’ e.g fans would also do the job) and purification (sucking the air through a filter to scrub out the pollutants/pathogens). I think both go some way to help this problem and just alone ventilation alone is more cost effective (table 1), however ventilation alone may not work in some instances. For instance, if the outside air is poor-quality (dense urban areas/near intense farming), or where there access to outside air is limited (high rise flats/offices where the windows don’t open), or for poorly-insulated buildings which are difficult to heat, so fresh air may be limited, it’s also hard to judge how much air needs to be replaced, which is where the CO2 and other monitors come in use.
Regarding the urban design idea, I’m not quite sure how effective this could be, a lot of the sources of air pollution are lots of individual sources, things like vehicle emissions, home heating, agriculture, which would make it hard to disperse by design, but it maybe more feasible with industry. But perhaps policy suggestions that control how much PM2.5/NO2 is emitted by industry might be warranted, which they could control by adding scrubbers/ filters to the outgoing air, if successful that might be applied to the smaller individual scale too. Thanks for these thoughts!
I am a big fan of ventilation and air quality as underrated issues! In addition to the many references you list, you might be interested in the following bits of info:
Although it’s a little hard to believe, there are many lines of compelling evidence indicating that air pollution isn’t just horrible for your long-term health, but also impairs one’s cognitive functioning on a short-term basis! See this website maintained by Patrick Collison for details. To the extent that this is true, it makes air pollution an even bigger threat to economic growth and human wellbeing.
As you probably have heard, OpenPhil is trying to expand their global health & development division to include charities centered on improving South Asian air quality, as this is a dire enough problem that it is probably competitive with Givewell top charities. Here is more detail on the south asian air quality issue.
This article summarizes an investigation by Johannes Ackva at Founders’ Fund into the effectiveness of their various climate charities. To my surprise (given how much society talks about climate change), air pollution has worse present-day impacts and is more actionable! To me, this fact really hammered home the importance and underratedness of air pollution.
Seconded that learning to do a great job of physically clearing pathogens from the air (with filters and UV light and etc) seems like a key technology to get familiar with for the purposes of GCBR mitigation, since it’s a physical block effective against a broad spectrum of threats. (For example, it would be just as easy for a physical filtering system stop a maliciously engineered nightmare virus impossible to vaccinate against, as for it to stop a common-cold rhinovirus.)
Thanks Jackson for forwarding on these interesting posts and info on this topic, I’m glad others have interest in this issue. I wonder if the topic is slightly underrated because its effects are often manifested as ‘long-lived’ insidious chronic issues, meaning that judging the cost-effectiveness of different interventions with relatively short randomly controlled trials is much more difficult compared to for instance infectious disease interventions. Perhaps that’s where your short-term cognitive effects might be a really useful diagnostic/measure of effectiveness of different interventions- so thanks for drawing my attention to that.
An effectiveness comparison between vaccination and air filtration/UV light methods as GCBR mitigation is a really good suggestion for future research. I agree that air filtration may prove to be pretty effective, especially given the time lag to develop & test vaccines too.
During the writing of this post I spoke to some engineers developing air purifiers for private sector, so if anyone has further interest in this topic in the future—I can put you in touch.