I’m a doctor working towards the dream that every human will have access to high quality healthcare. I’m a medic and director of OneDay Health, which has launched 53 simple but comprehensive nurse-led health centers in remote rural Ugandan Villages. A huge thanks to the EA Cambridge student community in 2018 for helping me realise that I could do more good by focusing on providing healthcare in remote places.
NickLaing
Karma: 14,220
Thanks for this ace article Morgan, I especially like “Fight against a sense of urgency when it builds up.”
I love this a lot and can already feel this among other orgs. A few people have said “Nick, think about how you could absorb more money soon” and I’ve been asked 3 times in the last 6 months by donors something like “could you take an extra 3-5 million dollars right now”.
These questions aren’t unreasonable, but the donors also need to be careful to not ramp up that urgency too much among us doers.
I feel like a lot of orgs will scramble to find ways to “absorb” money and grow. I think this will be a far bigger problem with the already-big BINGOs more than smaller orgs, because their claims to be able to absorb an extra 500 million or whatever will be both more public and more plausible.
We should be especially suspicious of orgs proposing brand new activities in the midst of this felt urgency that deviate from what they have been doing for some time.
My one disagreement is that “vaccine uptake and cash transfer programs in themselves could absorb a huge proportion of these funds, through government spending, GAVI, and organizations such as GiveDirectly.” I don’t think the Math maths on this front, and the CDG article doesn’t answer this question well either.
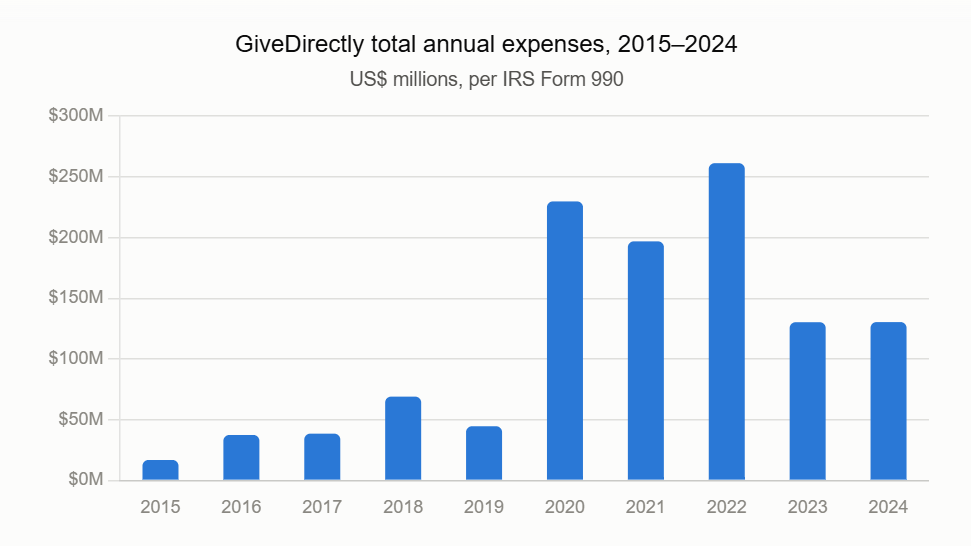
Looking at GiveDirectly specifically who might be the best placed org in the whole world to absorb lots of money cost-effectively and quickly, they say on their website they could spend 1.4 Billion in the next 3 years (sounds reasonable). The most they have ever spent in a year is 250 million dollars—I wouldn’t think more than doubling this year on year would be realistic.
The last thing I would want to do is give money to low-income governments to give away. This would be an absolute corruption fest and extremely poorly targeted. There’s already good evidence of this—look at Uganda’s recent cash giveaway program… GAVI could probably absorb a decent chunk, but we also don’t want to disrupt their program of forcing countries to slowly take over their own vaccine spend.
Super cool! Love the dashboard like @Mo Putera said, how did you make that beast?
Nice detailed feedback, makes a lot of sense. The 100 Karma cuttoff makes sense to me too, although I think reaching 100 Karma might be harder if posts are not displayed by default on the front page (but I’m sure you’ll see that). Can always change the threshold...
Yeah he’s doing great thanks @SiobhanBall. Good point about the economic system in behind which allows these innovations to flourish as well.
I don’t mind the idea, although I’m skeptical of this criteria ‘Selected posts to help us answer: how can we do the most good with our resources?’ For a start why not use the better-polling “selected posts that help us do more good”, which also helps with consistent CEA messaging.
I think many of the best posts don’t strictly follow that criteria. I agree it might be good to deprioritise these types of posts a bit you discuss...”EA community issues, share jobs, updates from organisations, ask for support with new projects, meet people ” but there are many others that inspire us or help us think differently that don’t stricly meet that criteria
These posts below for example are amazing (including classic posts), but don’t necessarily meet that criteria
https://forum.effectivealtruism.org/posts/wTXAbzbkAxZrLv5Cg/why-are-longtermists-so-much-less-focused-on-human
https://forum.effectivealtruism.org/posts/XuNBJL3EHqhFKLEGn/impact-requires-implementation-what-dispensers-for-safe
https://forum.effectivealtruism.org/posts/CmGPp5p9RvTLuuzbt/aim-high-even-if-you-fall-short
https://forum.effectivealtruism.org/posts/FpjQMYQmS3rWewZ83/effective-altruism-is-a-question-not-an-ideologyhttps://forum.effectivealtruism.org/posts/MGTzcHtwxpL6iXLJd/if-far-uv-is-so-great-why-isn-t-it-everywhere
I suppose it depends how widely that criteria is interpreted. Any great post can potentiall shift our hearts and actions to using resources better.
Never born, then maybe died twice
When the aliens come, they will wonder why we gave up our world so easily when there were so many warning shots.
Hey AI,vbiosec and American democracy makes sense but why a 10 year windowreproductive tech and emergingg farming tech?
I really don’t think things need to be seen as “canonical” to get widespread attention or adoption. I think you’re right though that its unlikely to be seen as a permanent/long term ranking that people refer to periodically. I can more see this kind of thing going vival or getting traction from time to timeif done in the right way.
Thanks for this great article, which leaves me with less hope than before I started reading it.
Like the author points out, none of these options have a lot of evidence that they have worked in the past, and the past often predicts the future. In fact things like Agriculture and Tourism have been tried as development routes by many governments without huge sucess.
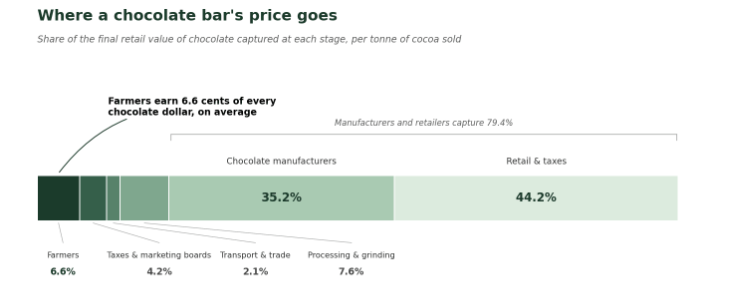
Of all these, I think for many African countries, value added agriculutre as an export focused business has decent potential. Uganda produces Cocoa, Milk and Sugar in abundance, yet still basically doesn’t make any chocolate and loses out from that big time ass this great graph shows.
A huge problem is that the protectionism of the West still severely limits this possibility. Tarriffs and import controls force poor countries to export these raw products to rich countries so they can make the chocolate and coffee themselves and make most of the money from it. The EUs agriculture import policy might have been one of the biggest constraints to African countries’ development for some time now.I think it can be easy to forget about the importance of educatoin deelopment too. As much as Taiwan’s chip boom was seeded by Taiwanese coming home, they had a world class education system (at least for the upper middle class) before that that took those engineers to the point that they were. The same can be said to some extent for the India’s IT growth. Without great education there isn’t a knowledge economy—you can’t export average knowledge services.
On Labour Migration, I still struggle to see how this can be a major driver of development. As a supplementary income source to help drive growth I think it is great, but how will just bringing in extra money (mostly to rich families) develop the country in the long term? Looking to the Phllipines again which is the darling of labor migration theory, they have a strong services export economy which was developed even while they were exporting all the labour. And both of those were built on a decent education system too.
I like the idea and I think its a great list. Given the failure and sort-of scandal around Dispensers for Safe Water, you might want to consider whether its a bit of a risk on a big portfolio like this. Nice job :)
After the World Cup result I think “lesser” suffices at this point ;)
I think the main point of the article is pretty clearly true and I appreciate the way it is written.
Part of the controversy might be because this is now the second article written here on the forum by a Fund Manager, which on an uncharitable reading could seem like they are saying that that Anthropic money will mostly go through us fund managers. We are the middle men with the power. So either appeal to fund managers like us or don’t bother. @SiobhanBall makes a similar point above.
Even if the advice is true, useful and given with a great heart (which I’m sure is the case here) it has a “gatekeepy” vibe for orgs not close to the “inner ring”.I have mixed feelings. On one hand this I agree that the advice is good and pretty common sense like you say (I certainly won’t be cold calling Anthropic staff and wouldn’t regardless). On the other hand when I read things like these...
”In the past year, donors working inside frontier AI labs have started routing large global health gifts to me to place.”and
”the most credible way to demonstrate this is to be highly rated by EA-aligned evaluators and grantmakers, already trusted by AI staff: Coefficient Giving, GiveWell....”
It feels like power over this money is likely to be heavily concentrated people in the “inner ring” who are already highly connected to Anthropic Staff and the current EA power structures. Power concentration combined with money concentration could be fine, but makes me nervous given both FTX, and that (Along with established funds) we are already seeing a bunch of new funds, led by people with not much experience, which might give out tens of millions of dollars without masses of accountability around them.
I love both of your ideas “Perhaps one aspect that could be valuable is to provide a list of more independent advisors?”. Sounds great, keeping in mind we would have to accept that if these advisors were truly “independent” from the EA circles, then they will be a bit less “EA” in their advice, and will more heavily weight less-EA considerations like orgs’ track record, local grounding and non DIY scale pathways.
I also like your other idea about talking with other big donors, and there are plenty of donors who give in the tens to hundreds of millions although not quite at GiveWell/Gates scale. Again the advice will be a little less EA aligned if moving outside the few core EA orgs for advice.
In addition to @huw’s great comment, there’s a branch of EA which focuses on well-being, and with that focus mental health interventions often look really effective. Check out the happier lives institute Huw mentioned, times the “WELLBY” and @MichaelPlant
Why would that be the case? I could work from my hut in Uganda on trying to shoot down Russian drones over Ukraine and it would not achieve anything. Obviously that’s a dumb strawmanb but just because people work on something doesn’t mean they will achieve anything.
Too late, but I would ask her to make the best case against immigration haha (much like you did with me and BINGOs 😅)
This is incredible, the best Global Health vid I’ve seen in ages so stoked! I know a vid is good when I feel comfortable imediately recommending it to non-EA friends.
I’m surprised it has so few hits, is there any marketing for this? Also is there a reason it isn’t on an official GWWC channel rather than a personal one?
Whoever disagreed with this should take a good hard look at themselves...
I see you as a founder regardless @huw. It’s a weird word but it’s well accepted in the social enterprise works at least that people who come in 2-3 years down the line and creatively grow an org are founders. I suppose it’s just semantics though.
I think its easy to underrate how much the moral compass of humanity can change over 75 years. And when it changes it can happen fast—thinking of civil rights movement and LGBTQ+ rights as well.
I think Alternative proteins could well become almost indistinguishable from meat, there will still need to be social/moral changes to encourage uptake, because people find it weird and unnatural. So mot sure how to weight on that front too.